





You asked, we answered
Questions for Steve
Terms & definitions
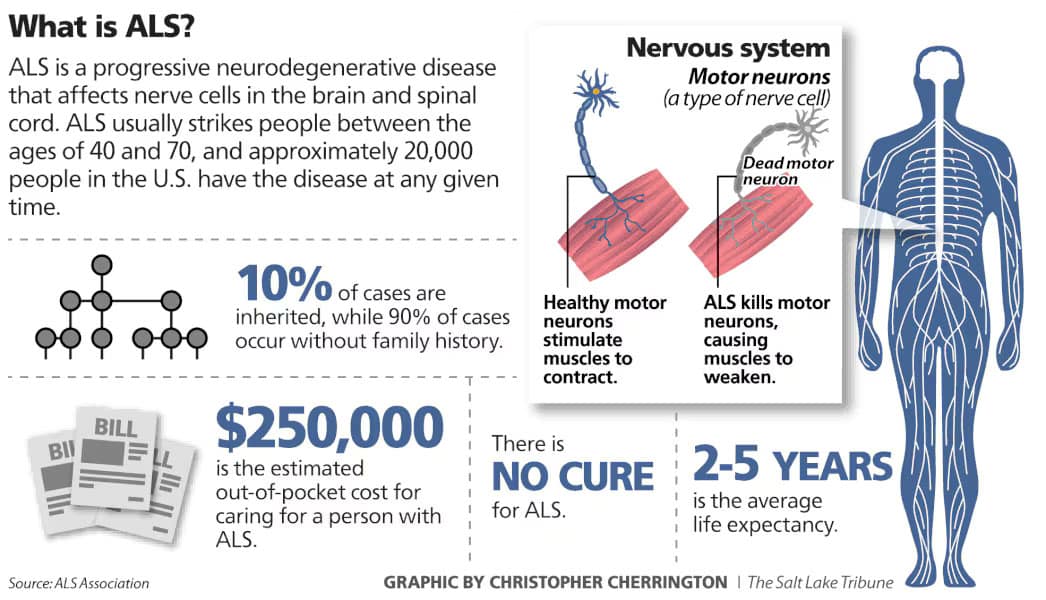
What is ALS?
Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig’s disease, is a progressive neurodegenerative disorder that affects motor neurons in the brain and spinal cord. These neurons control voluntary muscle movements such as walking, speaking, swallowing, and breathing. As the disease progresses, motor neurons degenerate and die, leading to muscle weakness, twitching, atrophy, and eventually paralysis[1].
Key Facts:
- Cause: The exact cause of ALS is unknown. Most cases are sporadic, but about 5–10% are familial, linked to genetic mutations such as in the SOD1 gene[2].
- Symptoms: Early signs include muscle weakness, cramps, twitching, slurred speech, and difficulty swallowing. As ALS advances, it affects mobility, speech, and breathing[3].
- Diagnosis: Diagnosis involves clinical evaluation, electromyography (EMG), nerve conduction studies, and ruling out other conditions[4].
- Progression: ALS is typically fatal within 2 to 5 years of symptom onset, although some individuals live longer. It does not usually affect cognitive functions, though some may develop frontotemporal dementia (FTD-ALS)[1].
- Treatment: There is no cure, but FDA-approved medications like riluzole and edaravone may slow progression. Supportive care includes physical therapy, speech therapy, and respiratory support[1].
For more detailed information, you can explore resources from:
- Mayo Clinic[3]
- The ALS Association[5]
- CDC National ALS Registry[2]
- National Institute of Neurological Disorders and Stroke (NINDS)[1]
References
[2] www.cdc.gov
[5] www.als.org
What is the ALSFRS-R score?
The ALS Functional Rating Scale – Revised (ALSFRS-R) is the most widely used clinical tool for assessing physical function and disease progression in individuals with amyotrophic lateral sclerosis (ALS). It was introduced in 1999 as an update to the original ALSFRS (1991) to better capture respiratory function alongside bulbar and limb domains[1].
Purpose
ALSFRS-R measures functional decline over time, helping clinicians monitor disease progression, guide treatment decisions, and evaluate interventions in clinical trials. It is considered a gold standard for ALS severity assessment[1].
Structure
- 12 items grouped into three functional domains:
- Bulbar: speech, salivation, swallowing
- Motor: handwriting, cutting food, dressing/hygiene, turning in bed, walking, climbing stairs
- Respiratory: dyspnea, orthopnea, respiratory insufficiency[2]
- Each item is scored on a 5-point scale (0–4):
- 0 = no function
- 4 = normal function
- Total score range: 0–48 (higher scores indicate better function)[3].
Clinical Use
- Tracks progression: average decline is about 1 point per month, though individual rates vary[4].
- Used in clinical trials, prognostic modeling, and staging systems like MiToS and King’s staging[3].
Limitations
- Does not fully account for differences in onset type (bulbar vs limb vs respiratory).
- Floor effect in advanced stages; extended versions (ALSFRS-EX) and self-explanatory versions (ALSFRS-R-SE) have been developed to address these issues[3].
For more details, see:
References
[1] resref.com
[2] www.mdcalc.com
[3] en.wikipedia.org
Here’s a detailed ALSFRS-R scoring table showing all 12 items and their 0–4 scoring criteria:
ALSFRS-R Scoring Table
| Domain | Item | Score 4 (Normal) | Score 3 (Mild Impairment) | Score 2 (Moderate) | Score 1 (Severe) | Score 0 (None) |
|---|---|---|---|---|---|---|
| Bulbar | Speech | Normal speech | Detectable speech disturbance | Intelligible with repeating | Speech combined with non-verbal | Loss of useful speech |
| Salivation | Normal | Slight excess saliva | Moderately excessive | Marked drooling | Severe drooling | |
| Swallowing | Normal | Occasional choking | Dietary consistency changes | Needs tube feeding for some | Tube feeding only | |
| Motor – Upper Limb | Handwriting | Normal | Slow or sloppy | Not all words legible | Able to grip pen only | Unable to grip pen |
| Cutting food & handling utensils | Normal | Some difficulty, no help | Needs help for some tasks | Needs help for most tasks | Unable | |
| Dressing & hygiene | Normal | Independent but slow | Needs some assistance | Needs much assistance | Totally dependent | |
| Motor – Lower Limb | Turning in bed | Normal | Somewhat slow | Needs occasional help | Needs frequent help | Unable |
| Walking | Normal | Early ambulation difficulty | Walks with assistance | Non-ambulatory | Unable | |
| Climbing stairs | Normal | Slow or mild difficulty | Needs assistance | Cannot climb stairs | Unable | |
| Respiratory | Dyspnea | None | Occasional shortness of breath | Shortness on exertion | Shortness at rest | Severe at rest |
| Orthopnea | None | Some difficulty lying flat | Needs extra pillows | Cannot lie flat | Unable | |
| Respiratory insufficiency | None | Intermittent BiPAP use | Regular BiPAP use | Continuous BiPAP use | Ventilator dependent |
Total Score Range: 0–48 (higher = better function).
What is FVC for breathing?
Forced Vital Capacity (FVC) is a key measurement in respiratory health that represents the maximum volume of air a person can forcefully exhale after taking the deepest breath possible. It is typically assessed using spirometry, a common pulmonary function test[1].
Purpose and Clinical Significance
- Diagnostic Role: FVC helps distinguish between obstructive lung diseases (e.g., asthma, COPD) where exhalation is impaired, and restrictive lung diseases (e.g., pulmonary fibrosis) where inhalation is limited[2].
- Monitoring: It is used to track disease progression, evaluate treatment effectiveness, and assess readiness for surgery or rehabilitation programs[2].
How It’s Measured
The test involves maximal inhalation followed by a forceful, complete exhalation until no more air can be expelled. This maneuver measures lung capacity and airflow dynamics[3].
FVC is often interpreted alongside FEV1 (Forced Expiratory Volume in 1 second) and the FEV1/FVC ratio, which are critical for diagnosing airflow obstruction[4].
Normal Values
- Normal FVC values vary by age, sex, height, and ethnicity. Typically, an FVC within 80–120% of predicted values is considered normal. Adult males often range between 4.8–6.0 L, and females between 3.2–4.5 L[5].
Key Formula
$ text{FVC} = text{Tidal Volume (VT)} + text{Inspiratory Reserve Volume (IRV)} + text{Expiratory Reserve Volume (ERV)} $ This reflects the total air expelled after a full inhalation[1].
For more details, see:
References
[1] www.respiratorytherapyzone.com
[4] www.lung.org
[5] spirometry.com
What is AAC software?
AAC (Augmentative and Alternative Communication) software is designed to support individuals who have difficulty with verbal speech due to physical, developmental, or cognitive challenges. Here’s a concise summary:
Purpose:
AAC software helps people communicate more effectively when speech is limited or absent. It can be used by individuals with conditions such as autism, cerebral palsy, ALS, stroke, or traumatic brain injury.
Types of AAC:
- Unaided AAC: Uses gestures, sign language, or facial expressions.
- Aided AAC: Involves tools or devices, including software on tablets, smartphones, or dedicated speech-generating devices.
Key Features:
- Text-to-Speech (TTS): Converts typed or selected words into spoken language.
- Symbol-Based Communication: Uses icons or pictures (e.g., PECS, Boardmaker) to represent words or phrases.
- Customizable Vocabulary: Allows users to tailor words and phrases to their needs.
- Touchscreen Interface: Often designed for ease of use with touch or switch access.
- Multilingual Support: Some AAC apps support multiple languages and dialects.
Popular AAC Software Examples:
- Communicator
- TD Snap
- Proloquo2Go
- TouchChat HD
- Snap + Core First
- Avaz
- Grid 3
Benefits:
Can be used in educational, clinical, and home settings.
Enhances independence and social interaction.
Supports language development and literacy.
What is AAC and what are common AAC myths? – Tobii Dynavox Global
